
ACDF
What Is ACDF?
Anterior cervical discectomy and fusion (ACDF) is the most common neck surgery. This procedure can be used to treat:
- Neck pain
- Myelopathy—compression of the spinal cord
- Radiculopathy—an inflamed or damaged nerve root that sends pain radiating to other parts of the body, usually from a disc herniation
The term ACDF means:
- Anterior: front of neck (access point for surgical incision)
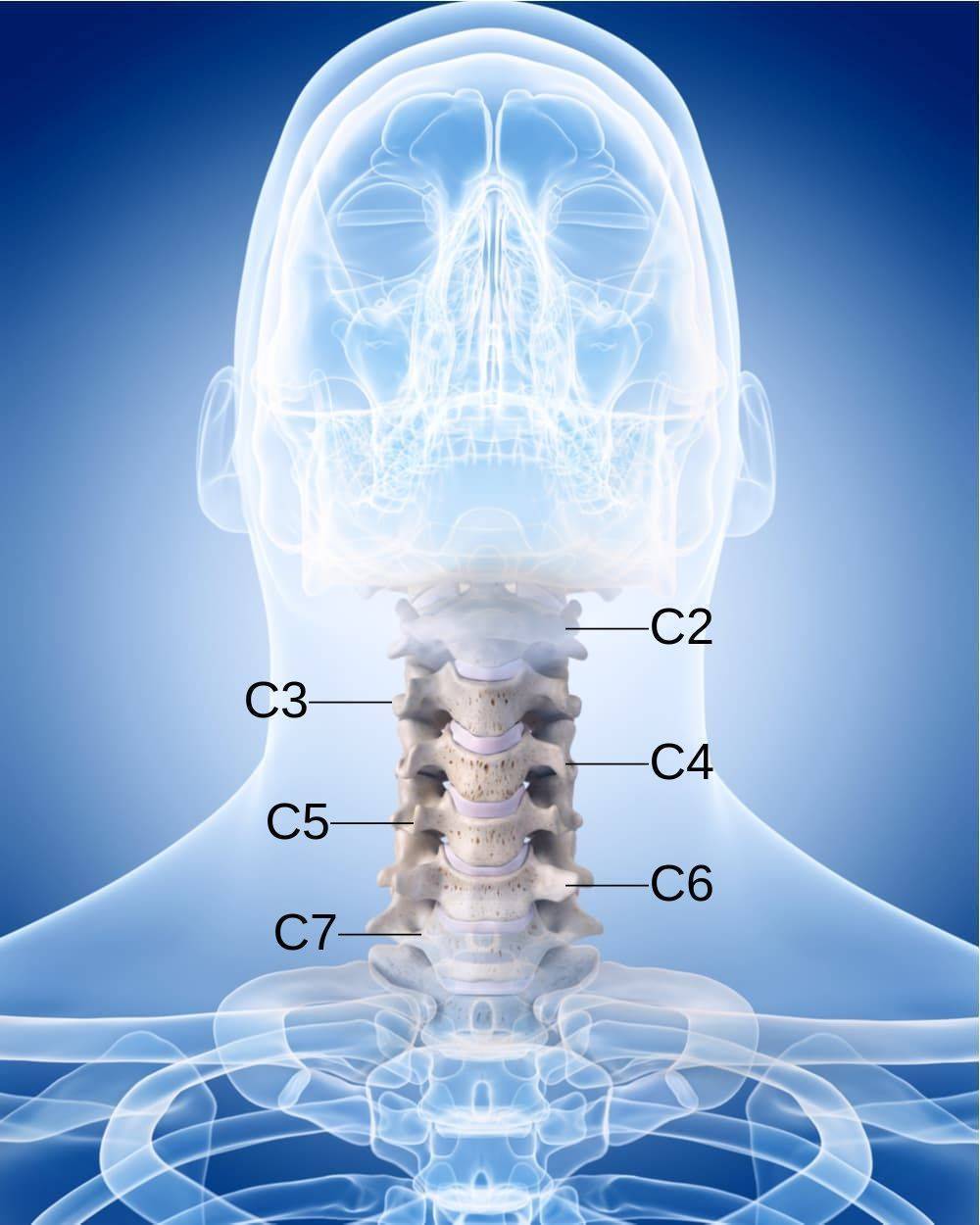
- Cervical: neck portion of spine
- Discectomy: removal or cutting out of the spinal disc between two vertebrae
- Fusion: fusion of spinal vertebrae by bone graft
 During ACDF surgery, the damaged vertebral disc or discs between one or more vertebrae are removed, relieving the pressure on the spinal cord and nerves. Then a bone graft is used to start the fusion process of the vertebrae, preventing further deterioration and stabilizing the cervical spine.
During ACDF surgery, the damaged vertebral disc or discs between one or more vertebrae are removed, relieving the pressure on the spinal cord and nerves. Then a bone graft is used to start the fusion process of the vertebrae, preventing further deterioration and stabilizing the cervical spine.
This procedure relieves the pressure on the nerves of the spinal cord and nerve roots, restoring neurological function to the arm and hand and relieving pain. Cervical fusion surgery and neck fusion are two other common names for this procedure.
ACDF Indications
Candidates for ACDF surgery include patients with one or more of the following:
- Myelopathy
- Pain and other symptoms that do not improve with physical therapy or medication
- Herniated disc – the soft inner layer of an intervertebral disc punches through the hard outer layer and can compress nerve roots
- Degenerative disc disease – a chronic condition in which vertebral discs dry out and shrink, which can lead to stenosis, herniation, bone spurs and joint inflammation
- Pinched nerve, which can cause:
- Significant weakness, numbness or tingling in the arm(s) or hand(s)
- Arm and neck pain, with arm pain worse than neck pain
- Cervical spine trauma
- Spinal stenosis—a narrowing of the spinal canal that can encroach upon the spinal cord or nerve roots
- Vertebral tumors
- Osteomyelitis—a bone infection
How the Procedure Is Performed
A minimally invasive incision is made in the front of the neck, which allows for minimal muscle dissection and bleeding to access the spine when compared to a posterior (from the back) approach. A posterior approach risks damage to the spinal cord, spinal nerves and neck muscles. The neck muscles, trachea and esophagus are moved aside to allow access to the affected area of the spine. A cervical discectomy – partial or complete removal of the herniated (protruding), injured disc or discs – is made. Any bone spurs that press on the nerve root will also be removed (foraminotomy).
After the discectomy, a bone graft is implanted between the two discs to restore the proper disc space height so the bones do not rub against each other and eventually fuse the two vertebrae together. An allograft (donor cadaver bone), an autograft—a graft from the patient’s own bone, usually from the hip—or a synthetic graft may be used. This bone graft acts as the scaffold or brace in which the patient’s own bone will grow.
Finally, a small metal plate is attached to the front of the vertebrae to help with the fusion process, as well as stabilize the spine. Complete fusion takes a few months to a year or two.
ACDF Recovery

ACDF is an outpatient procedure, and most patients are allowed to go home within a few hours after surgery. A follow-up appointment with the surgeon is normally scheduled for approximately two weeks after surgery.
Recovery time is usually four to six weeks, but varies by patient and if other medical conditions are present. A brace or cervical collar may be prescribed during the healing process to limit motion and provide support of the neck. Walking as soon as possible after surgery is important to help prevent blood clots and build strength. Physical therapy will be prescribed once the neck has healed.
Restrictions after ACDF surgery include:
- Use of non-steroidal anti-inflammatory drugs (NSAIDs) is prohibited for three to six months after surgery, as these medications may cause bleeding and interfere with bone healing and fusion. Tylenol may be used as well as narcotic pain relievers, but care needs to be taken with any opioid use due to their highly addictive nature.
- Smoking should be discontinued prior to surgery and prohibited after surgery. Smoking delays overall healing, increases the risk of post-surgical complications and inhibits bone fusion.
- Driving should be avoided for two to four weeks after surgery unless otherwise permitted by the surgeon.
- Sitting for long periods and long car rides should be avoided.
- Bending the head forward or backward should be avoided.
- Lifting anything heavier than five to ten pounds is restricted for the first few weeks after surgery.
- No housework and yard work unless otherwise permitted by the surgeon.
- Sexual activity should be postponed until the follow-up appointment unless otherwise permitted by the surgeon.
Some loss of range of motion may be present, but varies based on how many vertebrae are fused and by patient. Occasionally, better range of motion results. Arm pain is relieved in the vast majority of patients, though weakness and numbness may persist for weeks to months. Neck pain is also relieved in the majority of patients. Smoking greatly reduces the success of the procedure. Diligence with physical therapy is also a key component to a successful outcome.
If you think you may be a candidate for ACDF surgery, or if you’d like to learn more about options for neck and arm pain, contact us today for a consultation.


